Semaglutide vs. Tirzepatide vs. Retatrutide: The Weight Loss Numbers in Plain English
Three incretin drugs, three different receptor profiles, and three very different headline weight-loss numbers. Here is the cleanest plain-language comparison of semaglutide, tirzepatide, and retatrutide, plus the nuance people usually skip.
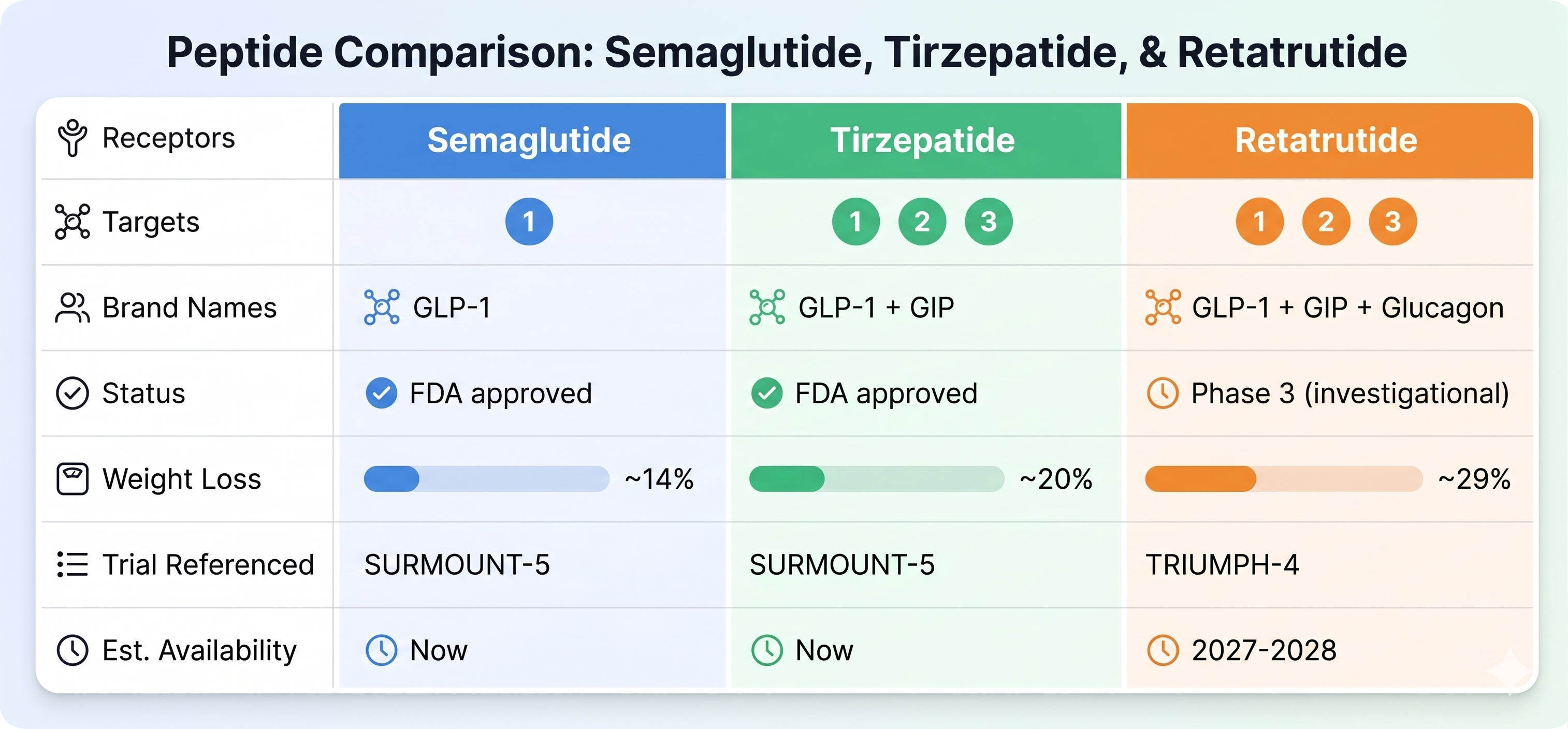
If you want the shortest possible version of the current GLP-1 weight-loss race, it looks like this:
- one receptor gets you roughly 14%
- two receptors gets you roughly 20%
- three receptors gets you roughly 29%
That framing is simple.
It is also only partly true.
The reason people keep repeating those numbers is that they capture the broad direction of the field:
- semaglutide opened the modern era
- tirzepatide pushed the ceiling higher
- retatrutide is the investigational candidate trying to push it higher again
But those percentages are not all drawn from one perfect apples-to-apples trial series.
So the best way to understand them is not as a single winner board, but as a plain-language map of where the market stands right now.
Step 1: what each drug actually is
Semaglutide
Semaglutide is a single agonist.
It activates GLP-1.
In the U.S., semaglutide is already approved and widely available:
- Wegovy for chronic weight management
- Ozempic for type 2 diabetes
Semaglutide is the drug that made GLP-1 weight-loss treatment mainstream.
Tirzepatide
Tirzepatide is a dual agonist.
It activates GLP-1 and GIP.
It is also already FDA approved:
- Zepbound for chronic weight management
- Mounjaro for type 2 diabetes
The simplest way to think about tirzepatide is that it took the semaglutide story and raised the weight-loss bar.
Retatrutide
Retatrutide is a triple agonist.
It activates:
- GLP-1
- GIP
- glucagon
That third receptor is the reason retatrutide gets so much attention.
GLP-1 and GIP are already familiar from semaglutide and tirzepatide.
Glucagon is the added piece that changes the conversation, because it is tied more directly to energy expenditure, not just appetite and satiety.
Retatrutide is not FDA approved. It is still investigational and legally available only through clinical trials.
The weight-loss numbers people are quoting
Here are the three headline numbers most people mean when they compare these drugs.
Semaglutide: about 14.9%
The landmark STEP 1 trial published in the New England Journal of Medicine reported average weight loss of 14.9% at 68 weeks with once-weekly semaglutide 2.4 mg in adults with overweight or obesity, compared with 2.4% for placebo.
That is the semaglutide number that anchored the modern obesity-treatment conversation.
Tirzepatide: 20.2% in SURMOUNT-5
In the head-to-head SURMOUNT-5 trial, tirzepatide reached 20.2% average weight loss compared with 13.7% for semaglutide at 72 weeks.
That is where the widely repeated “47% greater relative weight loss” line comes from.
The reason SURMOUNT-5 matters so much is that it is not just another placebo-controlled success story. It directly asked the question many people care about most:
How does tirzepatide perform against semaglutide in the same study?
And the answer was: better.
Retatrutide: 28.7% in TRIUMPH-4
In Lilly’s Phase 3 TRIUMPH-4 trial, participants taking retatrutide 12 mg lost an average of 28.7% of body weight at 68 weeks using the efficacy estimand.
The 9 mg dose reached 26.4%.
That is why retatrutide keeps getting described as the investigational drug most likely to reshape the obesity market once it reaches a decision point.
Those are enormous numbers.
They are also not the whole story.
The nuance people usually skip
This is the part that matters if you do not want to oversimplify the comparison.
These are not all from one perfectly matched trial design
Semaglutide’s 14.9% comes from STEP 1, a placebo-controlled landmark obesity trial.
Tirzepatide’s 20.2% vs 13.7% comes from SURMOUNT-5, a head-to-head trial against semaglutide.
Retatrutide’s 28.7% comes from TRIUMPH-4, a Phase 3 trial in people with obesity or overweight and knee osteoarthritis, not a direct head-to-head against tirzepatide or semaglutide.
That means the clean “one receptor vs. two vs. three” framework is useful for intuition, but not a perfect scientific ranking exercise.
It is directionally helpful.
It is not the same thing as one identical-trial scoreboard.
”More receptors” is not automatically a free upgrade
It is tempting to think:
more receptors = better drug
But that is too simple.
More receptor activity can mean:
- more pathways affecting weight loss
- potentially more potency
- but also more variables to manage
- more tolerability questions
- and less long-term real-world safety experience
That tradeoff matters.
Retatrutide’s side-effect profile is part of the story
The upside in TRIUMPH-4 was dramatic.
The side-effect picture was also more intense than what people are used to seeing in simpler “GLP-1 only” summaries.
According to Lilly’s TRIUMPH-4 release, the most common adverse events with retatrutide were gastrointestinal:
- nausea
- diarrhea
- constipation
- vomiting
- decreased appetite
Lilly also reported dysesthesia, an altered skin-sensation signal, in:
- 8.8% of participants on 9 mg
- 20.9% of participants on 12 mg
- compared with 0.7% on placebo
Those events were generally mild and rarely led to discontinuation, but they are still notable because dysesthesia did not become a headline feature of the earlier semaglutide narrative.
A similar signal also appeared in Lilly’s Phase 3 diabetes program for retatrutide, though at lower rates.
So if retatrutide eventually reaches market, the conversation will not just be “it works better.”
It will also be:
how much better, for whom, at what dose, and with what tolerability tradeoff?
Where each drug stands right now
If you want the market snapshot in one section, it is this:
Semaglutide
- the established modern GLP-1 benchmark
- FDA approved
- broad real-world use
- still highly effective
- no longer the ceiling
Tirzepatide
- the current approved leader in weight-loss magnitude
- FDA approved
- directly beat semaglutide in SURMOUNT-5
- still the most important approved comparator in the field
Retatrutide
- still investigational
- strongest weight-loss headline of the three
- mechanistically the most ambitious because of added glucagon activity
- likely to be one of the most important obesity-market catalysts if late-stage development continues to hold up
So which one is “best”?
That depends on what you mean by best.
If you mean:
most established and widely used
the answer is semaglutide.
If you mean:
strongest approved weight-loss data today
the answer is tirzepatide.
If you mean:
investigational drug most likely to reset expectations again
the answer is retatrutide.
Those are three different questions.
The plain-language takeaway
Semaglutide proved the category.
Tirzepatide moved the approved standard forward.
Retatrutide is the investigational triple-agonist trying to move it again.
The easiest shorthand is:
- semaglutide: around 14.9%
- tirzepatide: around 20.2%
- retatrutide: around 28.7%
But the better way to say it is:
These drugs do not just differ by weight-loss percentage.
They differ by:
- receptor profile
- approval status
- trial design
- tolerability
- and how much real-world evidence exists today
That is why the most honest ranking is not “1st, 2nd, 3rd.”
It is:
- semaglutide is the proven single-agonist benchmark
- tirzepatide is the current approved leader
- retatrutide is the Phase 3 investigational drug most likely to reshape the market if the remaining data hold
Sources
- New England Journal of Medicine / PubMed: STEP 1 semaglutide trial
- FDA: Wegovy cardiovascular-risk indication and current indication summary
- FDA: Zepbound approval for chronic weight management
- Eli Lilly: SURMOUNT-5 complete results
- Eli Lilly: TRIUMPH-4 Phase 3 retatrutide results
- Eli Lilly: retatrutide Phase 3 diabetes results and dysesthesia signal
- Lilly FAQ: what to know about retatrutide